
Table of Contents
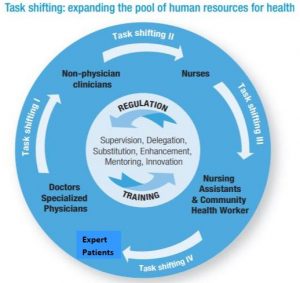
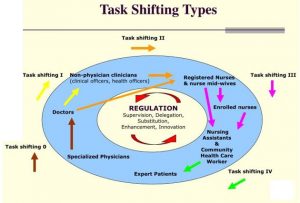
What is Task Shifting?
- According to World Health Organization, Task shifting means, “the rational re‐distribution of tasks among health workforce teams. Specific tasks are moved, where appropriate, from highly qualified health workers to health workers who have fewer qualifications in order to make more efficient use of the available HRH.” (WHO, 2008)
- Task shifting is process of delegation whereby tasks are moved, where appropriate or from highly specialized workforce to less specialized health workers
- It is a great option and method to enhance efficiency on delivery of health care services
- As for an example: when doctors are in short supply, a qualified nurse or the local health worker could often prescribe and dispense medicine or say attend the medical emergency.
- Task shifting is done for the better use of human resource and the uninterruptable service provision
Rise of the Concept of Task Shifting:
- Task shifting was first developed as the strategy in context of HIV and AIDS treatment.
- The overall shortage of health workforce was the major problem in tackling the HIV/AIDS pandemic and universal access of essential health.
- Shortage of the health worker was global problem in health sector.
- Thus, task shifting strategy was developed so as to expand capacity of existing health personnel, and add new cadres of workers
- WHO, together with the US President Emergency Plan For AIDS Relief (PEPFAR) and the Joint United Nations Programed on AIDS (UNAIDS), developed global guidelines for task shifting which were launched during the first ever Global Conference on Task Shifting in Addis Ababa on 8-10 January 2008.
- Many countries have adopted the task shifting strategy.
- Besides HIV/AIDS treatment task shifting strategy has been adopted in providing other health services like maternal and reproductive health services as well.
Global Status of Health Workforce:
- The world is experiencing a chronic shortage of well-trained health workers.
- A total of 57 countries, mostly in sub-Saharan Africa but also including Bangladesh, India and Indonesia, face crippling health workforce shortages.
- WHO estimates that more than 4 million health workers are needed to fill the gap
- The global deficit of doctors, nurses and midwives is at least 2.4 million
– Source: WHO, 2007
Objectives of Task Shifting:
- To increase the productive efficiency i.e. rise in number of health care services provided at given quality and cost
- To reduce the time needed to scale up the health workforce
Rationale of Task Shifting/Why is Task Shifting Needed:
Task shifting is necessary and of urgent need, especially in developing countries:
It is needed in order to:
- Address low human resources for health (HRH)
- Increase coverage of health services with limited human resource
- Address poor HRH retention, especially in rural and less developed areas
- Reduce the burden of specific human resource
- To increase the efficiency of health service delivery
- More preference to the urban sector by the health professional causing health workforce crisis and inequity
Advantages of Task Shifting:
a) Solution to health worker crisis
- Shortage of physicians, nurses, pharmacists, and other clinicians and health personnel makes people rely on traditional models of healthcare delivery or prevents them from seeking health
- Task shifting/ shifting of task at such scenario would help in meeting the health needs of the people and also reduces the health gap.
b) Cost saving and improve in efficiency
- Task shifting is not only necessary to fill the HRH gap but it is also important from economic point of view
- It helps in reducing the cost
- Task shifting supports the optimized utilization of the manpower thereby reducing the cost
- Task shifting also motivates the staffs, increasing their zest to work harder.
- Reduction in health worker training and bill costs
c) Coverage and access to health
- Task shifting increases number of services provided at a given cost and quality
- Increases patient access
- Remote areas where the health services are not easily available and medical professional do not dare to go, task shifting makes the health services accessible in such areas
- The local health worker can be trained and scaled up
- These also helps in reducing the burden at specific health centers/facilities.
- Gives positive contribution to overall health system strengthening.
Limitations of Task Shifting:
- Shifting of responsibilities from higher level professional to lower level can create conflicts in between the professionals. Clash of ego is quite common.
- Doubts/lack of satisfaction regarding treatment among the general public may be also seen.
- For task shifting, training of the staffs and health workers is required, which can in turn increase the immediate cost/investment.
- In some cases, quality of treatment might get compromised as some health workers may be less experienced and might have less knowledge/expertise on areas outside of their expertise.
- Harm or risk to client safety.
- Continuous supervision is most to ensure quality treatment.
- Task shifting can be effective for short run. However, it may not be a sustainable method for the long run.
Case study in Uganda:
Background:
Uganda is a land-locked country in Eastern. Uganda has poor health indicators. Diseases related to poverty, such as malnutrition and diarrhea, are common; and chronic diseases, such as diabetes and hypertension, are on the rise. In addition, Uganda has a generalized HIV epidemic. HIV prevalence was about 6 % (2006) and was the most common cause of death among all age groups.
Rationale:
The HIV epidemic has made task shifting a necessity for HIV- and AIDS-related services. The AIDS related cases were initially managed at facilities with specialists (e.g., immunologists and physicians). However, with time, number of people living with HIV/AIDs increased.
Introduction of Task shifting:
Doctors and the specialists were not adequate which resulted in doctors without specialization to take care of AIDS patients. Furthermore, lay service providers, such as counselors, treatment supporters, and People Living with HIV (PLHIV) have taken on greater roles in all aspects of prevention, treatment, care, and support of those infected and affected by HIV. The National STI and AIDS Control Program has developed treatment guidelines that various levels of health cadres are using to roll out antiretroviral treatment (ART) as well. At the Infectious Disease Institute (IDI) in Mulago Hospital, nurses have been trained and offered guidelines to manage AIDS patients who come for check-ups. Majority of the people had supported the idea. Task shifting in Uganda is seen for Mental Health Service, management of adult and adolescent illness as well.
References and for More Information:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5223454/
http://www.who.int/healthsystems/task_shifting/en/
http://www.who.int/healthsystems/task_shifting_booklet.pdf
http://www.uniteforsight.org/health-workers-course/module4
https://human-resources-health.biomedcentral.com/articles/10.1186/s12960-017-0200-9
https://www.medscape.com/viewarticle/705727
http://journals.plos.org/plosone/article?id=10.1371/journal.pone.0174631
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3503551/
http://www.who.int/evidence/resources/country_reports/TaskShiftingfullreport2010.pdf
http://www.healthpolicyplus.com/archive/ns/pubs/hpi/1112_1_Uganda_Case_Study_FINAL_5_05_10_acc.pdf